What Is Endoscopic Ultrasound and When Is It Needed?
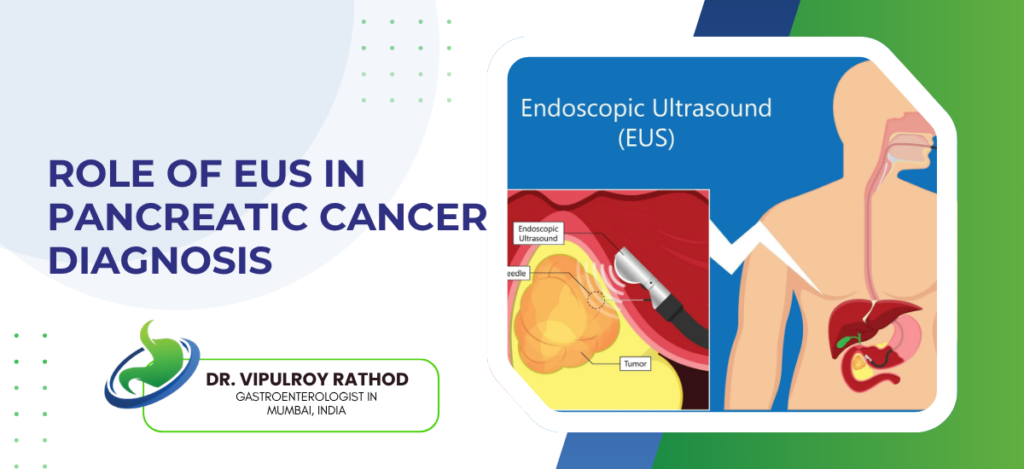
Endoscopic ultrasound puts a high-frequency ultrasound probe on the tip of a flexible endoscope and images organs from inside the GI tract, millimetres from the target rather than through layers of skin and fat from outside. It’s needed when CT or MRI can’t give a clear answer, when deep tissue biopsy is required without surgery, or when cancer staging depends on detail external imaging consistently misses. We use it because it sees what other scans don’t, and in pancreatic, biliary, and upper GI disease that difference changes treatment decisions regularly. According to Dr. Vipulroy Rathod, Gastroenterologist in Mumbai, “EUS is the investigation that closes the gap between what CT shows and what’s actually there, and in pancreatic, oesophageal, and gastric disease that gap is often the difference between the right treatment plan and the wrong one.” What Is EUS and How Does It Work? Standard endoscopy looks at the surface. EUS looks through the wall and beyond. Not a small difference when you need to know what’s happening in the pancreas or inside a lymph node CT flagged but couldn’t characterise. Mechanism: Ultrasound transducer on the scope tip, positioned inside the stomach or duodenum, images wall layers, lymph nodes, vessels, and adjacent organs at 5 to 12 MHz frequencies, resolution that shows individual tissue layers CT physically cannot distinguish from the outside. Biopsy: Needle passes through the GI wall into a pancreatic mass, lymph node, or submucosal lesion under real-time ultrasound guidance, no external incision, tissue result often changes the entire treatment plan because imaging alone can suggest but biopsy confirms. Procedure: Sedation, scope through the mouth into stomach or duodenum for upper EUS, through rectum for rectal staging, 30 to 60 minutes total, home same day, and most patients are surprised it was less involved than they expected going in. Safety: Complication rate under 1% for diagnostic EUS, 1 to 2% for FNA, serious events like perforation are rare when someone experienced is doing it, and the information gained almost always outweighs the small procedural risk in patients where EUS is genuinely indicated. EUS delivers information no other single investigation provides in one session. Specialist in endoscopic ultrasound uses it as the primary tool for conditions where it genuinely changes what happens next. When Is EUS Actually Needed? Not for every GI complaint. Specific decision points where its accuracy changes the management plan. Outside those, it’s not the right investigation. Pancreatic: Any pancreatic mass, cyst, or suspected cancer needs EUS because CT misses sub-2 cm tumours routinely, and if you’ve had persistent upper abdominal symptoms with a normal CT that doesn’t explain them, EUS is where the answer usually sits rather than another round of the same scan. Staging: Confirmed oesophageal, gastric, pancreatic, or rectal cancer needs EUS for T and N staging because tumour depth and nodal involvement measured on EUS consistently outperform CT, and getting the stage wrong means the patient ends up on a treatment pathway that doesn’t match their actual disease. Submucosal: Lumps found underneath the surface on routine endoscopy, GISTs, leiomyomas, carcinoid tumours, need EUS to characterise layer of origin, size, and internal features before anyone decides whether to remove or watch, and standard endoscopy alone cannot make that call. Biliary: Bile duct stones missed on ultrasound, suspected bile duct cancer, ampullary tumours, all evaluated more accurately on EUS than external imaging, and EUS-guided FNA of bile duct masses gives tissue diagnosis that ERCP brushings miss in a meaningful proportion of cases. EUS earns its place when the answer genuinely matters for treatment. Read more on EUS in pancreatic cancer to see how it changes diagnosis and staging decisions specifically in pancreatic disease. Why Choose Dr. Vipulroy Rathod for Endoscopic Ultrasound? Dr. Vipulroy Rathod has been performing diagnostic and therapeutic EUS since 1998 at Fortis Hospital Mulund. Over 30 years of case volume across pancreatic, biliary, oesophageal, gastric, and rectal EUS. First Indian to receive the FASGE fellowship. 35 countries worth of physicians trained in EUS technique and clinical interpretation. Patients arrive with inconclusive CT reports and months of unanswered questions. Most leave with a finding, a tissue diagnosis, and a clear next step nobody else had been able to provide. Book your consultation today with one of India’s most experienced EUS specialists for accurate diagnosis and intervention. Book Appointment Call now Frequently Asked Questions What is the difference between EUS and regular endoscopy? Regular endoscopy sees the surface lining while EUS images through the wall and surrounding structures using ultrasound for deeper diagnostic detail. Is EUS painful? EUS is performed under sedation and most patients experience minimal discomfort during and after the procedure. Can EUS detect cancer that CT missed? Yes, EUS detects pancreatic and GI tract lesions under 2 cm that CT regularly misses and provides tissue biopsy in the same session. How long does an EUS procedure take? EUS with or without biopsy typically takes 30 to 60 minutes including sedation and recovery time. Reference links- Endoscopic Ultrasound Indications and Guidelines — American Society for Gastrointestinal Endoscopy EUS in GI Disease Diagnosis — World Gastroenterology Organisation
What Is Endoscopic Ultrasound and When Is It Needed? Read More »