Patient Profile
Patient Name: Rajan S. (name changed for confidentiality)
Age: 52 | Gender: Male | Location: Thane, Maharashtra
Referred By: General Surgeon — open surgery had been recommended prior
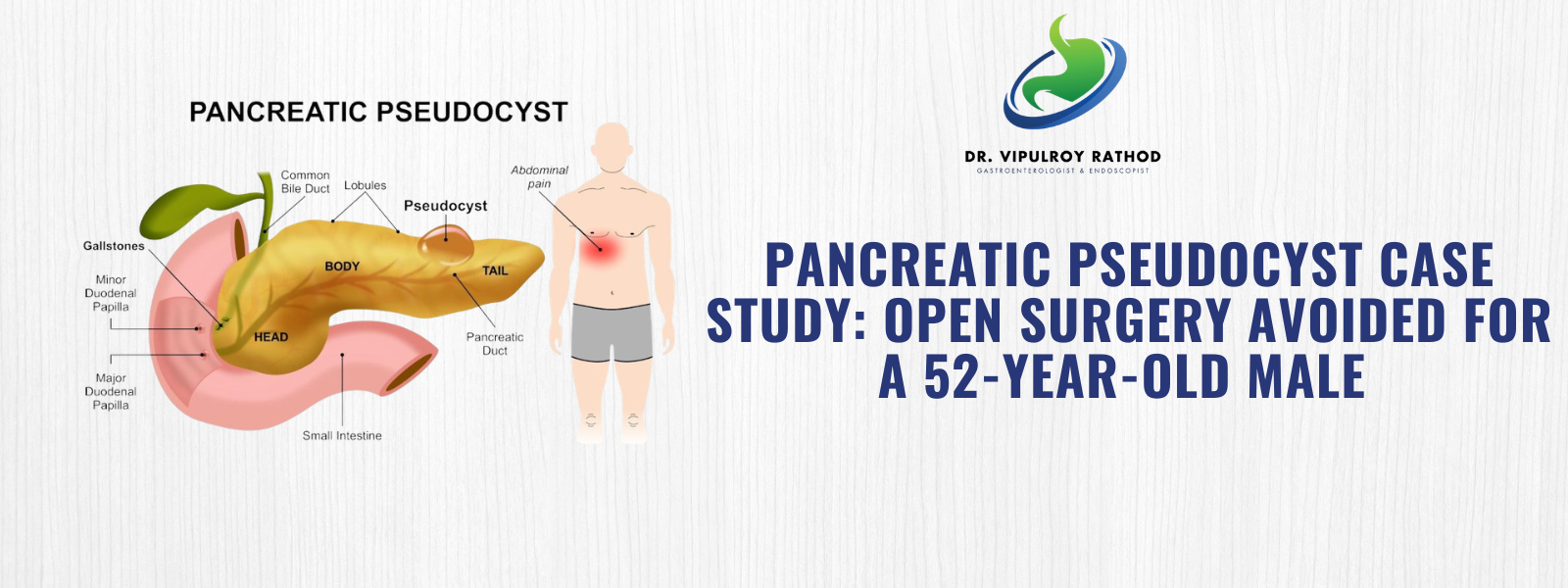
Tests: CT scan confirmed 6 cm pancreatic pseudocyst | Acute pancreatitis 6 weeks prior
Complaint: Severe epigastric pain, nausea, loss of appetite — 3 weeks duration
Patient Background:
Rajan S., a 52-year-old working professional from Thane, Maharashtra, visited Dr. Vipulroy Rathod at Fortis Hospital Mulund with concerns about severe upper abdominal pain that had disrupted his daily life for nearly three weeks. Like many patients dealing with complications of acute pancreatitis, Rajan found himself unable to eat, unable to work, and increasingly anxious about his condition.
Despite a CT-confirmed diagnosis and a referral for open abdominal surgery, his family was not ready to accept surgery as the only option. A search for the best Gastroenterologist Mumbai led them to Dr. Vipulroy Rathod — pioneer of EUS in South Asia and the most experienced endoscopic ultrasound specialist in India, with over 20,000 procedures to his name.
Symptoms
- Severe epigastric pain — persistent upper abdominal pain for three weeks
- Nausea and vomiting — inability to retain normal meals
- Loss of appetite — significant reduction in food intake
- Abdominal fullness — pressure sensation from cyst mass effect on surrounding organs
Diagnostic Method
- CT scan review — confirmed 6 cm pseudocyst adjacent to the posterior gastric wall
- Endoscopic Ultrasound (EUS) — high-resolution imaging to map cyst boundaries and vessel proximity
- Fluid aspiration — confirmed benign pseudocyst, ruling out cystic neoplasm
Disease Diagnosed
Rajan was diagnosed with a symptomatic pancreatic pseudocyst following acute pancreatitis. At 6 cm, the cyst compressed surrounding structures, causing all presenting symptoms. Patients in this condition are often referred to a GI specialist in Mumbai for a minimally invasive opinion before any surgical decisions are made.
Risks if Left Untreated:
- Rupture and peritonitis
- Pancreatic abscess
- Bile duct compression and jaundice
Treatment Plan
As one of the most experienced endoscopists in Mumbai, Dr. Vipulroy Rathod determined that the pseudocyst’s position made it ideal for EUS-guided transmural cystogastrostomy — a minimally invasive technique creating a drainage channel between the stomach and the cyst, avoiding open surgery entirely.
Why EUS-Guided Drainage Was Chosen Over Open Surgery
1. No Surgical Incision Performed entirely through the mouth — no abdominal opening, no general anaesthesia, no scar.
2. Faster Recovery Days vs. 4–6 weeks of surgical recovery. Rajan was back at work in one week.
3. Safer Post-Pancreatitis Avoids the inflamed post-pancreatitis surgical field, significantly reducing risk.
4. Proven Efficacy Over 90% resolution rate — the internationally recommended first-line treatment for pancreatic and biliary conditions.
How the Procedure Was Performed
- Rajan was placed under conscious sedation — no general anaesthesia required.
- A linear array echoendoscope was passed through the mouth to the posterior gastric wall overlying the cyst.
- Colour Doppler imaging confirmed a safe, avascular transmural window for needle access.
- A 19G EUS needle punctured the cyst; aspiration confirmed correct entry.
- A double-pigtail stent was deployed between the stomach wall and cyst, establishing continuous internal drainage.
Procedure Summary
- Procedure: EUS-Guided Transmural Cystogastrostomy
- Duration: 55 minutes | Anaesthesia: Conscious sedation
- Hospital Stay: Overnight — discharged the following morning
“When I pioneered EUS in South Asia in 1998, patients with large pseudocysts had no option but surgery. Today, we can resolve most in a single session. Any patient told they need surgery for a pancreatic cyst should seek an EUS specialist’s opinion first.” — Dr. Vipulroy Rathod, FASGE | Gastroenterology Specialist in Mumbai | EUS Pioneer, South Asia
Post-Surgery Guidelines
- Liquid and soft diet for 48 hours, advancing as tolerated
- Avoid alcohol and high-fat foods for the full 8-week stent period
- CT follow-up at 2 weeks to confirm cyst regression
- Stent removal at 8 weeks once resolution is confirmed on imaging
Outcome
| Timepoint | Result |
|---|---|
| 24 hours | Dramatic pain relief — ate and drank comfortably for the first time in three weeks |
| Day 1 | Discharged from hospital — no wound care required |
| 1 Week | Returned to full normal activity and work |
| 2 Weeks | CT confirmed cyst reduced from 6 cm to under 1 cm |
| 8 Weeks | Stent removed endoscopically. No complications |
| 6 Months | Complete resolution confirmed. Zero recurrence. No surgical scar |
Long-Term Expectations With dietary modifications and alcohol avoidance, Rajan’s prognosis is excellent. Annual follow-up with Dr. Rathod will monitor pancreatic function and digestive health long-term.
Patient Feedback
“When we were told I needed open surgery, we were frightened. We found Dr. Rathod online, and from the first consultation we knew we were in the right hands. He resolved three weeks of “ — Rajan S.,
Suffering from a similar condition? Book a consultation with Dr. Vipulroy Rathod today.